|
|
|
|
Chapter 1
|
|
Each vertebra has a hole in it, so when vertebrae are stacked together, they provide a hard, bony tunnel through which the spinal cord passes. This is called the spinal column. In this way, the spinal cord is protected from damage. (See figure 1.1.) There are four sections of your spine. The top is the cervical (SURR-vick-ull) section, which makes up your neck. The next down is the thoracic (thor-ASS-ick) section, which runs to your waist level. The lumbar (LUMM-bar) level is next and is your lower back. And last is the sacral (SAY-crull) part, which is your tailbone. (See figure 1.2.) |
|
|
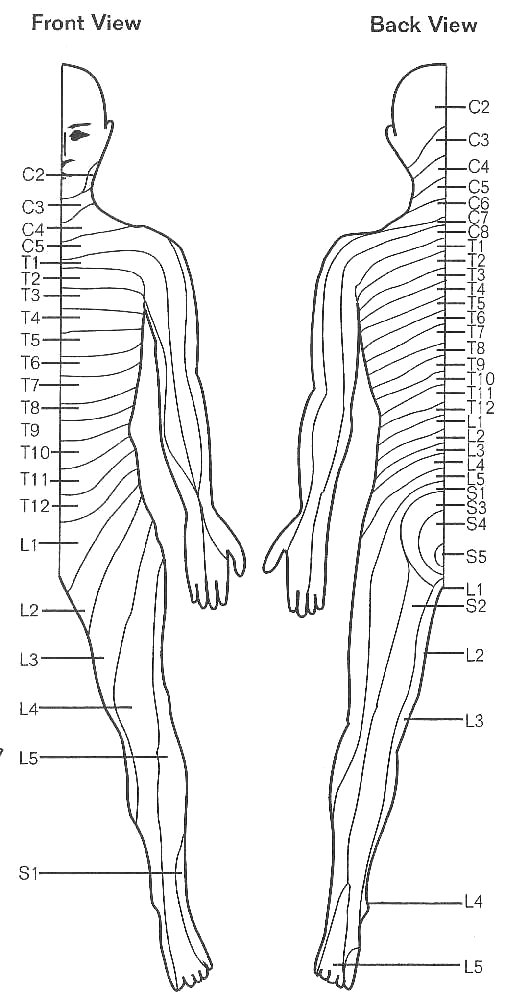
There are eight pairs of nerves and seven vertebrae in the cervical section of your spine. In this case, the nerves numbered C1 through C7 are above the corresponding numbered vertebrae. C8 then slips through between the C7 and T1 bones. For the thoracic and lumbar sections, each of the numbered nerves lies below the corresponding numbered vertebra. There are 12 thoracic vertebrae and 5 lumbar vertebrae. At the lower end of your spinal cord (below the second lumbar vertebra), the nerves travel long distances before they exit the spine. This is because the spiral cord itself ends much higher than where your tailbone marks the lower end of your spine. This makes the lower lumbar and sacral nerves look like a horse’s tail inside the spiral column. It is known as the cauda equina (CODD-ah eh-QUINE-ah), which means "horse’s tail" in Latin. Your sacral section is really only one piece of bone with five nerve pairs coming out through holes in it. |
|
|
|
The spinal cord is the communicating link between the spinal nerves and the brain. The nerves that lie only within the spinal cord itself are called upper motor neurons (UMNs). These run only between the brain and the spinal nerves. The spinal nerves branch out from the spiral cord into the tissues of your body. Spinal nerves are also called lower motor neurons (LMNs). (See figure 1.3.) In movement, the brain sends messages through the spinal cord (UMNs) to the spinal nerves (LMNs). The LMNs then carry these messages to the muscles to coordinate complicated movements such as walking. In this way, the brain can influence movement. In sensation, information is collected by nerves in your body and sent up the spinal cord to the brain. This allows conscious awareness of feelings such as heat or cold. |
|
|
You may wonder how the spinal cord keeps these messages from getting confused, with all the running back and forth between brain and body. The motor nerves and the sensory nerves carry messages in different nerve fibers. Within the cord itself, the nerve fibers are combined into spinal tracts. Each tract carries messages one way, either up for sensation or down for voluntary movement. They are similar to the lanes on a freeway. (See figure 1.4.) |
|
|
|
You might want to make your own map of
|
|
|
Most spinal injuries damage both UMNs and LMNs. A complete injury cuts or squeezes all the UMNs running down the spinal cord. This disrupts the connection between the brain and the parts of the body below the injury. LMNs below your spinal cord injury are not damaged. Because LMNs carry reflex actions, the reflexes below the level of injury are still in working order. This is a UMN injury. (See figure 1.7.) The reflex action that the LMNs carry out below the level of injury may still work, but there is one problem. In reflexes, the brain keeps control on how much your nerves react. In a UMN injury, control by the brain no longer exists because messages from the brain can’t get through the point of injury. The LMNs act by themselves, causing reflexes without limit. One example is spasticity (spa-STI-si-ti). Spasticity is the uncontrolled movement of your arms of legs. See more about spasticity in the chapter on Nerves, Muscles & Bones. |
|
LMN injuries are a different story. This kind of injury is found for the most part at the lower tip of the spinal cord, or the cauda equina. Damage to the cauda equina impairs reflex actions. This is because the cauda equina is made up entirely of LMNs. Other UMNs and LMNs above the injury are still in good shape. (See figure 1.8.) Spasticity is not found in LMN injuries as it is in UMN injuries, because muscles governed by these LMNs tend to shrink or atrophy (AT-row-fee). This is because these muscles no longer have any nerve contact to stimulate them. Stated simply, a UMN injury is one where the UMN pathway is broken and the LMNs below the injury are intact and spasticity is noted. An LMN injury, usually at the cauda equina, abolishes nerve contact with muscles controlled below the injury and no spasticity develops. It is important for you to know which type of injury you have, because how your spinal cord injury is managed will differ depending on that fact. |
|
The information provided here is for general purposes only. The material is not a substitute for consultation with your health-care provider regarding your particular medical conditions and needs. The information provided does not constitute a recommendation or endorsement by Beyond SCI with respect to any particular advice, product, or company. Beyond SCI assumes no legal liability or responsibility that the information appearing on this website is accurate, complete, up to date, or useful for any particular purpose. Please note that information is constantly changing; therefore, some information may be out of date since the last update.