|
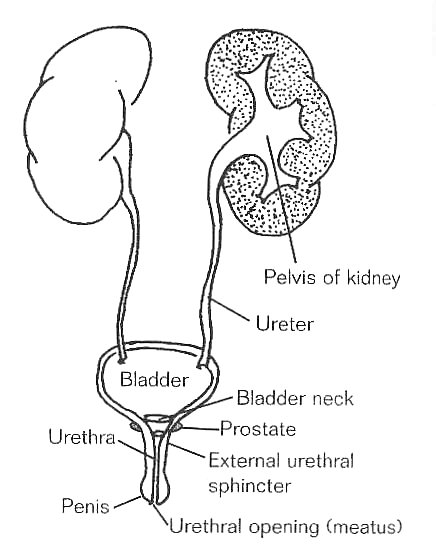
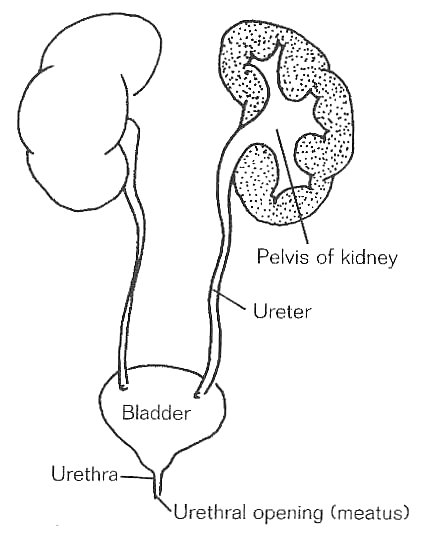
The primary differences between the male and female urinary systems are the length of the urethra and the presence of a prostate in the male. Otherwise, the systems are the same.
The kidneys remove waste and excess water from your blood stream and process them into urine. The urine then flows down the ureters (which are small tubes) to your bladder. The bladder is a muscular sac that stretches to hold urine until you are ready to void (urinate). When voiding occurs, the bladder (also called the detrusor muscle) contracts and the sphincter (which is a circular muscle acting as a gate) opens. Urine then process through the urethra and you urinate.
Urination calls for a finely balanced coordination of bladder and sphincter muscles. This coordination involves both voluntary and involuntary (or automatic) control by the nervous system. When the bladder becomes full, nerve impulses are sent to the sacral level of the spinal cord, and then sent to your brain to let you know that your bladder is full. At that time, you can decide to either urinate or hold the urine. This is the part under voluntary control. If you want to void, the brain will send messages back to the urinary system. The involuntary part involves the opening of the sphircter muscle and the bladder muscle contraction.
Changes in Bladder Function After SCI
Following SCI, nerve impulses from the bladder can no longer get to and from the brain to let you sense that your bladder is full or to let you void. There are two general kinds of bladder dysfunction that can occur, depending on your level of injury. Because there can be individual variations, you will probably have some tests to diagnose your particular bladder type. Although these are described below, it is important that you not depend on labels to describe your bladder.
Upper Motor Neuron Bladder (Reflex or Spastic Bladder)
The upper motor neuron (reflexic or spastic) bladder tends to hold smaller volumes of urine than before an injury. Just like your other muscles, your bladder muscles may have spasms and contract on their own. The result is that you may have frequent, small urinations with varying amounts of voluntary control, depending on the severity of your neurologic injury. This activity is common in SCI above the sacral level.
Lower Motor Neuron Bladder (Flaccid Bladder)
In the lower motor neuron (flaccid or areflexic) bladder, the bladder muscle has lost its ability to contract and can be easily stretched, allowing large volumes of urine to accumulate in the bladder. Because the muscle does not contract, urine may leak from the bladder when it is over-distended (overfilled). The urine "spills over" like a glass that is too full of water. This bladder activity is common when SCI affects the sacral cord--cauda equina, the spinal nerves below the sacral cord.
In both types of bladders, sensation of fullness is impaired.
BLADDER FUNCTION TESTS
There are a number of tests that can evaluate the structure and function of the urinary system. Because they are all commonly done, the tests are described here to prepare you in advance. You may have one or several of them.
Imaging Procedures
KUB (Kidneys, Ureters, Bladder)
Plain x-ray visualizes the abdomen and surveys the urinary tract.
Ultrasound
In the ultrasound, sound waves (like sonar) are bounced off tissue surfaces, and an electronic picture is produced on a screen. Variations in the image can detail the structures or anatomy and thus define problems.
This test is useful in identifying tumors, cysts, and stones in the urinary tract. It also is used to measure the prostate, testicles, and other organs in the abdomen.
Renal Scan
The purpose of a renal (REE-null) scan is to assess the function and the blood supply of the kidneys. It is done by injecting a radioactive substance into a vein and then "reading" counts over the kidneys. The amount of radioactivity is extremely low.
Intravenous Pyelogram (IVP)
An IVP is an x-ray study in which an intravenous injection of contrast material containing iodine is given. The contrast is excreted by the kidneys and shows up on x-ray. A series of films is taken to show the size, shape, and working order of the kidneys, ureters, and bladder. It can also show the size and number of kidney stones, if present.
PLEASE NOTE that if you have ever had an allergic reaction to the IVP dye, be sure to tell your physician.
Your bowel needs to be empty for this test, so do a good bowel program the evening before or the morning of the test. You may also have to refrain from eating and drinking the night before the test. The nursing staff will let you know if other preparation is necessary.
Cystogram
In this test, contrast material is injected into the bladder via a catheter. This test shows the size and shape of the bladder, as well as if urine moves backward through the system from the bladder up to the kidneys (reflux). This condition is due to excess pressure in the bladder, and is one cause of kidney damage, which needs to be detected and treated early.
Bladder Filling Studies
Cystometrogram
A cystometrogram (siss-toh-METT-roh-gram) (CMG) shows how your bladder reacts when it is filled with either carbon dioxide (CO2) or water. This mimics the way it would usually react when filled with urine. A urethral catheter is inserted for this test. The test measures the amount of pressure that builds in your bladder. With this information your practitioner can help plan a bladder program best suited for you.
Urodynamics
Urodynamics (yurr-oh-die-NAMM-icks) is a broad term that refers to a series of diagnostic techniques used to evaluate the bladder. Tests that may be part of this urodynamics evaluation include a cystometrogram, measurement of urethral pressures, as well as EMG (electromyograph) of the external sphincter.
This comprehensive study will assist in planning the best bladder management program for you. If there are changes in your bladder function over time, you may need this study repeated.
Cystoscopy
Cystoscopy (siss-TOSS-koh-pee) involves the urologist looking at the inside of your urethra and bladder through a lighted, hollow, specialized telescope inserted through the urethra. This is used in diagnosing and sometimes treating problems occurring inside the bladder.
Other Laboratory Tests
There are a number of tests evaluating the blood and urine that show how your urinary system is functioning:
Creatinine (kree-AT-en-een) clearance
This test involves collecting all of your urine for a 24-hour period. It is an important indicator of kidney function.
Urine cultures
A urine specimen is sent to the laboratory to look for bacteria. When a sensitivity test is also ordered, specific antibiotics that kill these bacteria can be determined.
Urinalysis
Urine is analyzed for a number of different chemical and cellular products.
Blood ureanotrogen (BUN) and creatinine: This blood test monitors renal function.
BLADDER MANAGEMENT
There are a number of basic goals in bladder management:
- Have low bladder volumes
- Have low bladder pressures
- Avoid infections
- Keep your skin dry
Bladder volumes are kept low by:
- Watching your fluid intake
- Routinely emptying your bladder
If you have an incomplete injury, you may with time regain some or all voluntary control of your bladder.
If you have a complete injury, one or a combination of the following bladder emptying techniques will become part of your bladder management program.
Bladder Emptying Techniques
Intermittent Catheterization
A small rubber or plastic tube is inserted into the bladder to drain urine several times a day. We refer to the process as an intermittent catheterization program, or ICP. The nursing staff generally does ICP initially. As you become more involved in your care, you or your attendant will be taught so you can continue this at home.
If you are managing your bladder with ICP, you will be asked to keep your bladder volume around 300 to 500 ml/cath. Adjust the frequency and the interval of catheterizations and the fluid intake to produce a minimum of 1,500 cc/day of urine output. You should catheterize at least four times per day and, depending on your fluid intake, you may catheterize more often.
Important note: More than 500 cc in your bladder overstretches your bladder muscle and makes you prone to infection or reflux. (See the section in this chapter on Avoiding Infections.
Indwelling Catheter
Two types of continuous drainage are urethral (foley) and suprapubic catheters. A foley catheter is a hollow tube with a balloon on the end so when inflated it will stay in your bladder. This is placed through your urethra (urine channel) and is usually changed one time per month. A suprapubic catheter is placed in your bladder through a small opening in your lower abdomen. This is a surgical procedure. Once the opening is made you or your attendant can change the catheter about once a month, just like a foley. This catheter also has a balloon to keep it in your bladder.
Stimulated Voiding
Some bladders can be mechanically stimulated to empty. Just as a spastic muscle may move when tapped or brushed, so may a UMN bladder. "Reflex voiding" may be induced by tapping over the lower abdomen or tugging on pubic hairs.
Spontaneous Voiding
Some UMN bladder muscles spontaneously contract. For those who have bladders that trigger on their own or who have had a sphincterotomy (SFINK-turr-AH-tom-ee, surgery to open the bladder "gate"), wearing an external collecting device or condom catheter will keep you dry. There are many different types of condoms, and your SCI team will work with you to find the best device for you.
Keeping Bladder Pressures Low
High bladder pressures before the bladder empties can cause urine to "back up" (reflux) into the kidneys, causing damage. Two such conditions are:
- Irritable bladder--loss of bladder compliance, meaning the bladder has lost its elasticity, so that high pressures are generated with increasing volumes of urine. It is not advisable to use valsalva or crede maneuvers to empty the bladder with known high pressures.
- Dyssynergia (DISS-inn-URR-jah)--the bladder contracts but the sphincter will not open. It is like trying to press the air out of a mattress with the plug closed. Autonomic dysreflexia can also occur with dyssynergia. (See the chapter on Autonomic Dysreflexia.) To keep pressures low, keep your volumes low and treat the dyssynergia. Dyssynergia can be treated by either the use of medication to relax the sphincter or by surgery to open it up.
Avoiding Infections
- Maintain a consistent fluid intake to "wash out" bacteria and to limit stone formation.
- Empty your bladder routinely and prevent overdistension. More than 500 cc can weaken your bladder muscle in two ways. First, the muscle cells cannot fight off infection as well. Second, the muscle cannot contract as tightly and leaves behind a pool of urine in which bacteria can grow.
- Sterile catheterization is performed while you are in the hospital. You will be taught a "clean" technique for home management before discharge. In some instances you may do a clean catheterization while in the hospital.
- If you are taking any medication related to your bladder management, make sure you follow the practitioner’s recommendations.
Keeping Your Skin Dry
The best way to keep your skin dry is to carefully follow your bladder management program.
- Routinely empty your bladder by the method that works best for you.
- Manage your fluid intake.
- Wear appropriate appliances. These include condoms/external devices or padding specific to you.
- Avoid infections. Infections may make your bladder irritable, which can cause frequent incontinence between intermittent catheterization or leakage around foley or suprapubic catheters.
- Change your clothes as soon as they are wet.
PROBLEM SOLVING
People with SCI are at risk for infection because mechanical methods are needed to empty the bladder. Infections are caused by bacterial growth. Three sites of infection common to SCI are the kidney, bladder, and testicles.
A kidney infection is called pyelonephritis (PIE-ell-low-neff-RIGHT-iss); a bladder infection is called cystitis (siss-TIE-tiss); and an infection involving the testicles is called epididymitis (epp-eh-DID-ee-MIGHT-uss).
Table 6.A will help you understand these infections and diagnostic tests and treatments that may be required.
|