|
|
|
|
Chapter 7
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
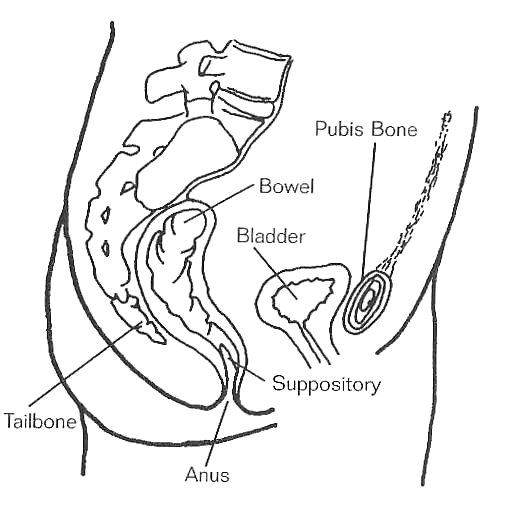
Your diet, the amount of exercise you do, and the regularity of your bowel movements play an important role in keeping you healthy. The following is a description of the digestive system and how some parts can affect your bowel movements. (See figure 7.1.)
|
|
|
|
||
A bowel program is the total combination of diet, exercise, fluids, medication, and scheduled bowel care. The goals of your bowel program are to prevent bowel accidents (unplanned bowel movements), to produce bowel movements at regular and predictable times, and to minimize bowel-related complications.
Bowel care is the scheduled process of starting and assisting your body to have a bowel movement. Bowel care is part of the bowel program. Bowel care is the procedure for assisting bowel movements that can be learned and followed in a series of steps.
Good control of your bowels after a spiral cord injury is possible with planned bowel care as part of a bowel program. Keeping your bowel emptied on a regularly scheduled basis to prevent chronic over-distention is the goal. Using an abdominal binder to support the abdomen may be helpful.
To stimulate peristalsis (wave-like movement of the intestines), you may use a rectal suppository, mini-enema, and/or digital stimulation of the rectal muscles. Scheduled bowel care can be done on a commode, on a toilet, or in bed with pads, whichever works best for you.
The types of things you will need included in your bowel care as part of your overall bowel management program will be best determined by the type of bowel you have following your SCI, whether it is reflexic or areflexic. The rehabilitation nurse and your health-care provider will work with you to establish the most effective bowel care routine. The following is a description of things and techniques that are commonly used in bowel care regimes. Table 7.A lists some medications that may be prescribed as part of your bowel program.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||
If you have sufficient upper extremity function, you will learn to do your own bowel care. If you are not able to do your own bowel care, you will learn to instruct others in the process.
Do your bowel care about 30 to 45 minutes after a meal or hot drink, because this stimulates peristalsis to promote stool movement in your colon. If you use intermittent catheterization procedure (ICP) to empty your bladder, you should do it before bowel care.
|
|
|||
|
||||
|
|
Diarrhea is frequent loose or watery stools, which may cause unplanned bowel movements and accidents.
Constipation is a common condition in which stool does not pass as often, as fast, or as completely as we usually expect. The stool may be hard and dry. It is sometimes hard to determine if you are constipated until you have had incomplete results or no results after 2 or more episodes of bowel care. Be sure you know the amount of stool produced with each bowel movement.
An impaction is a partial or complete blockage in the intestine by stool.
Rectal bleeding is seen as bright red blood on your stool, toilet paper, or glove.
See the chapter on Autonomic Dysreflexia.
|
Neurogenic Bowel: What You Should Know: A Guide for People with Spinal Cord Injury
Constipation and Spinal Cord Injury: A Guide to Symptoms and Treatment
Purchase
PVA Distribution CenterDownload: www.pva.org
PO Box 753
Waldorf, MD 20604-0753
(888) 860-7244
Bowel Management Programs: A Manual of Ideas and Techniques
Purchase
Accent Press
Accent Special Publications
Cheever Publishing, Inc.
PO Box 700
Bloomington, IL 61702
(309) 378-2961
Taking Care of Your Bowels
Purchase
VA San Diego Healthcare System
Spinal Cord Injury Center (128)
3350 La Jolla Village Dr.
San Diego, CA 92161
(858) 552-8585
Taking Care of Your Bowels-The Basics
Taking care of Your Bowels-Ensuring Success
Purchase
Northwest Regional Spinal Cord Injury SystemDownload: depts.washington.edu/rehab/sci/
University of Washington
Rehab Medicine Clinic
1959 NE Pacific
Seattle, WA 98195
(800) 366-5643
Home Care Manual for Spinal Cord Injury
Purchase
Santa Clara Valley Medical Center
Education Dept.
751 S. Bascom
San Jose, CA 95670
(408) 885-2000
"Preventing Secondary Medical Complications: A guide for personal assistants to people with spinal cord injury"
Purchase
Research ServicesDownload: www.spinal.uab.edu
UAB, Department of Physical Medicine and Rehabilitation
619 19th Street, South, Room 529
Birmingham, AL 35249
(205) 934-3283
Bowel Management in Spinal Cord Injury: Fact Sheet #10
Purchase
Arkansas Spinal Cord Commission
1501 North University,
Suite 470
Little Rock, AR 72207
(501) 296-1788
SCI Video Access, a lending program of information videos
Spinal Cord Injury Network
3911 Princeton Drive
Santa Rosa, CA 95405
(800) 548-2673 or (707) 577-8796
The information provided here is for general purposes only. The material is not a substitute for consultation with your health-care provided regarding your particular medical conditions and needs. The information provided does not constitute a recommendation or endorsement by Beyond SCI with respect to any particular advice, product, or company. Beyond SCI assumes no legal liability or responsibility that the information appearing on this website is accurate, complete, up to date, or useful for any particular purpose. Please note that information is constantly changing; therefore, some information may be out of date since the last update.